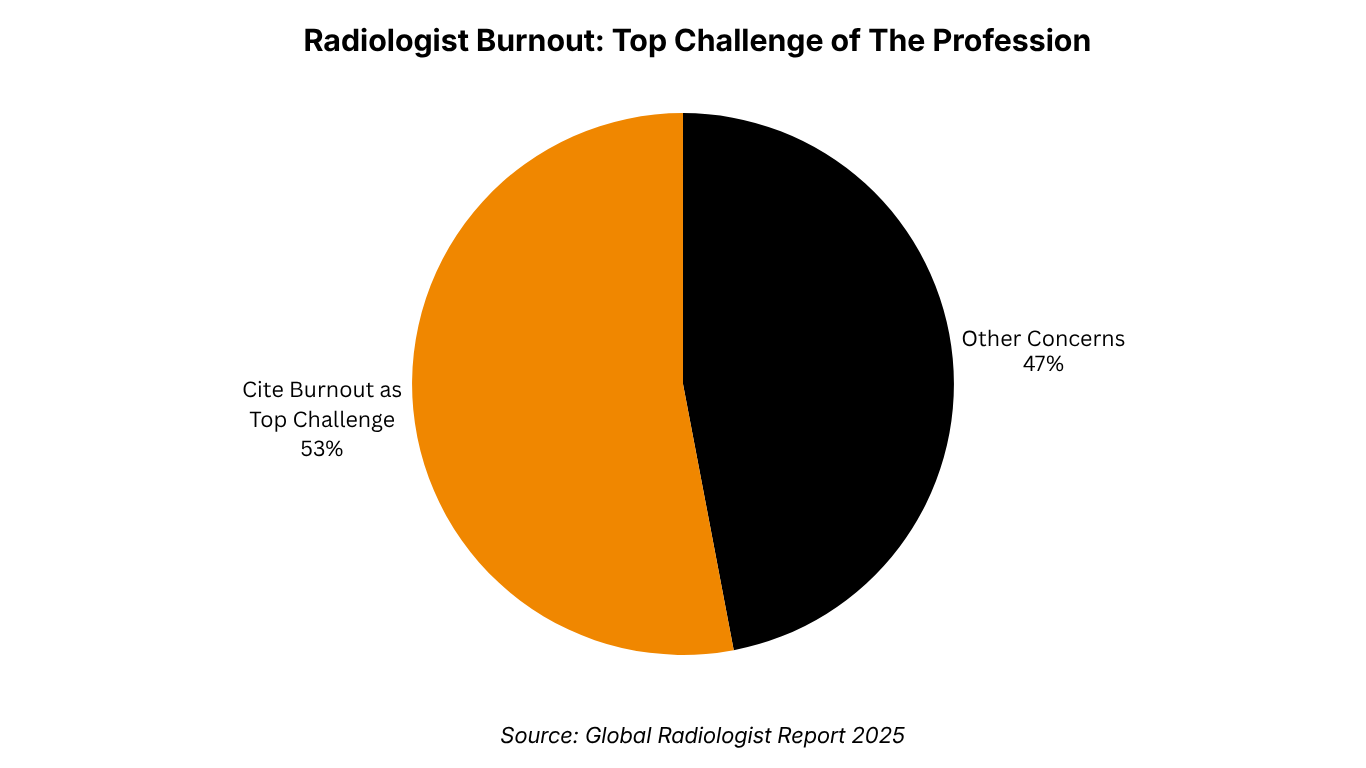
53%
of radiologists cite burnout as the #1 threat to the profession
ISO 13485: 2016 Certified - Software as a Medical Device (SaMD)

Burnout is not a personality problem. It is a documentation problem. And the fix is already here.
Ayesha Khan · June 2026 · 7 min read

53%
of radiologists cite burnout as the #1 threat to the profession
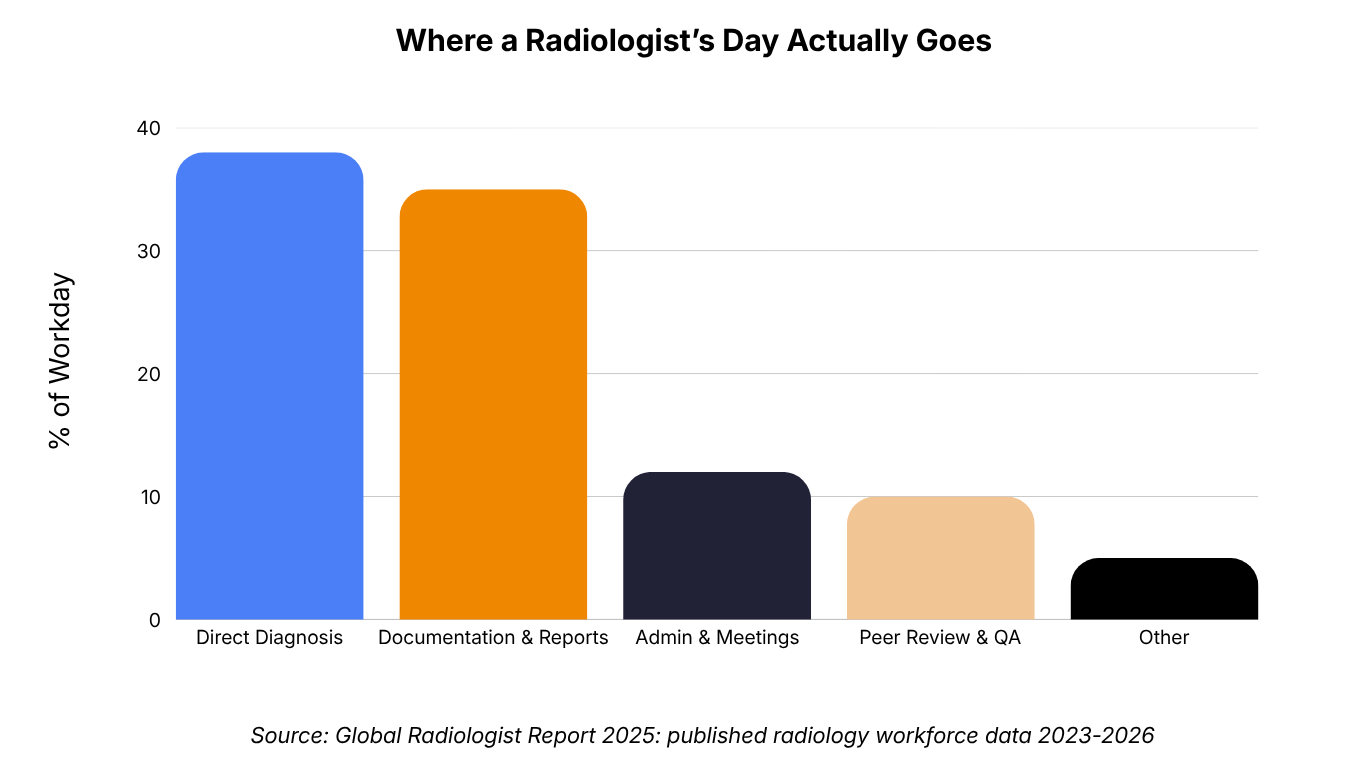
30–40%
of a radiologist's day spent on documentation
80%+
of patient episodes depend on an imaging report
<10s
PRAID AI Scribe: dictation to structured draft
Sources: Global Radiologist Report 2025; published radiology workforce data 2023–2026; PRAID AI Scribe Product Brief
Picture this: a senior radiologist, three hours into a Saturday shift. She has reviewed 47 scans. She has diagnosed two probable malignancies, flagged a subtle intracranial bleed, and caught a fracture a junior missed. None of that is why she is exhausted. She is exhausted because she still has to write 47 reports.
That tension — between the intellectual work radiologists trained for and the documentation work that fills their days — is now a measurable crisis. According to the Global Radiologist Report 2025, 53% of radiologists name burnout as the single biggest threat to the profession's future. That is not a majority. That is a supermajority. And when you dig into the cause, documentation is almost always in the frame.
This post is about that problem, and about why AI-powered radiology reporting is not just a productivity upgrade but a workforce retention strategy that hospital leadership cannot afford to ignore.
The medical conversation around burnout often drifts toward personal resilience, mindfulness apps, flexible scheduling, wellness programmes. These are not useless. But they are addressing the symptom while leaving the cause untouched.
Research into radiology workforce data from 2023 to 2026 consistently points to the same root cause: 30 to 40% of a radiologist's working day is consumed by documentation, not diagnosis. For a profession that requires years of subspecialty training and continuous exposure to complex pathology to stay sharp, spending a third of every shift typing — or worse, reformatting dictation into structured templates — is a profound mismatch of skill and task.
The documentation load is also unevenly distributed. High-volume teleradiology operations, multi-site hospital groups, and pathology departments — where structured reporting has historically lagged behind radiology — carry disproportionate administrative weight. When a radiologist is reading 80 to 100 studies per shift, the reporting overhead does not scale linearly. It compounds.
You cannot solve a documentation crisis with a meditation app. You solve it by automating documentation.
Burnout does not happen in a vacuum. It sits inside a broader workforce crisis that makes each individual radiologist's output more critical, and each departure more costly.
The WHO's Global Health Workforce Statistics and the ACR's 2024 Workforce Survey both point to a structural imbalance: demand for imaging reads is growing at roughly 3 to 5% per year, driven by ageing populations, expanding screening programmes, and improved access to imaging in emerging markets. Radiologist training pipelines, by contrast, grow slowly. The result is a widening gap between what the system needs and what it can deliver.
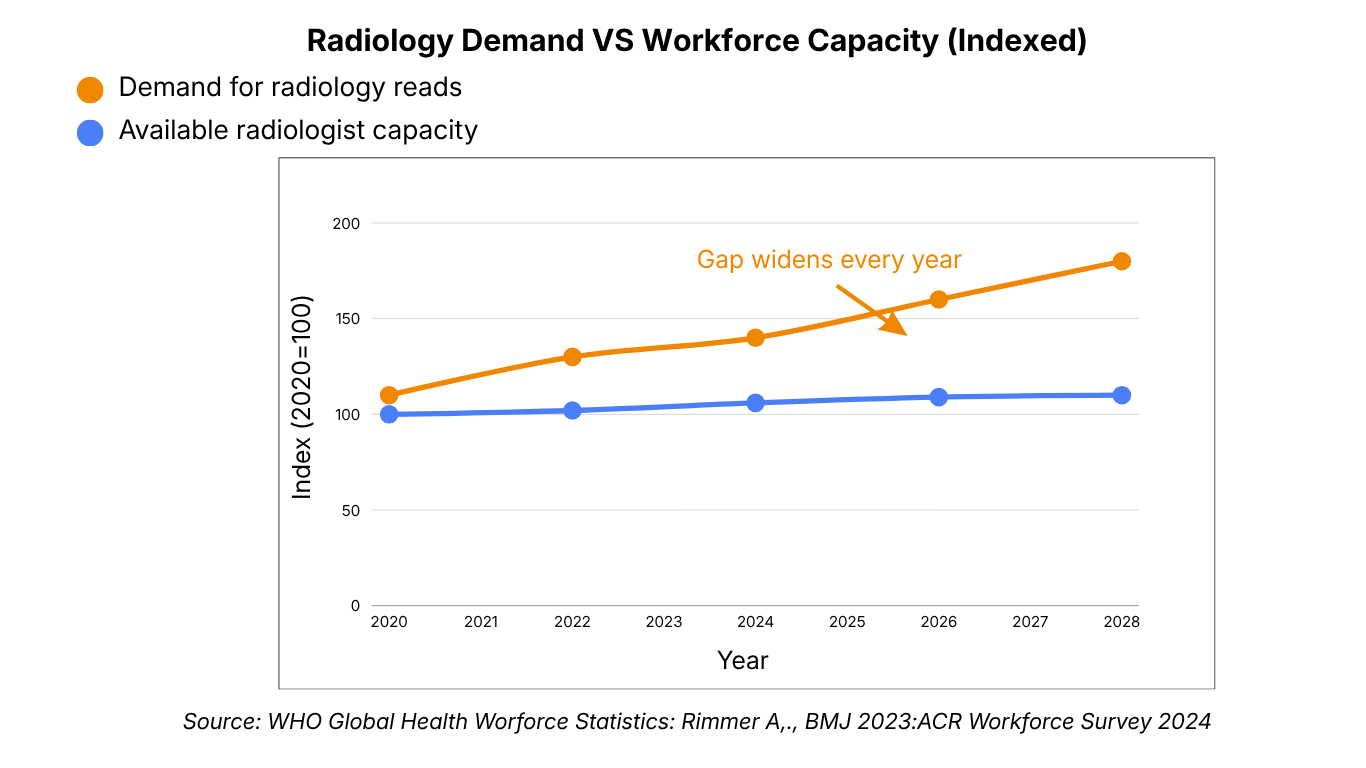
In this context, losing experienced radiologists to burnout is not just a human resources problem. It is an operational and clinical risk. A BMJ analysis (Rimmer, 2023) noted that radiologist attrition in high-income countries is increasingly being filled by locum and agency cover, at significantly higher cost and with lower continuity. The economics of ignoring burnout are catching up with hospital finance teams.
The calculus, then, is straightforward: every hour returned to a radiologist from documentation is an hour that stays in diagnosis, that reduces error risk, and that makes that radiologist more likely to stay in the role. AI medical report generation is not a nice-to-have. It is retention infrastructure.
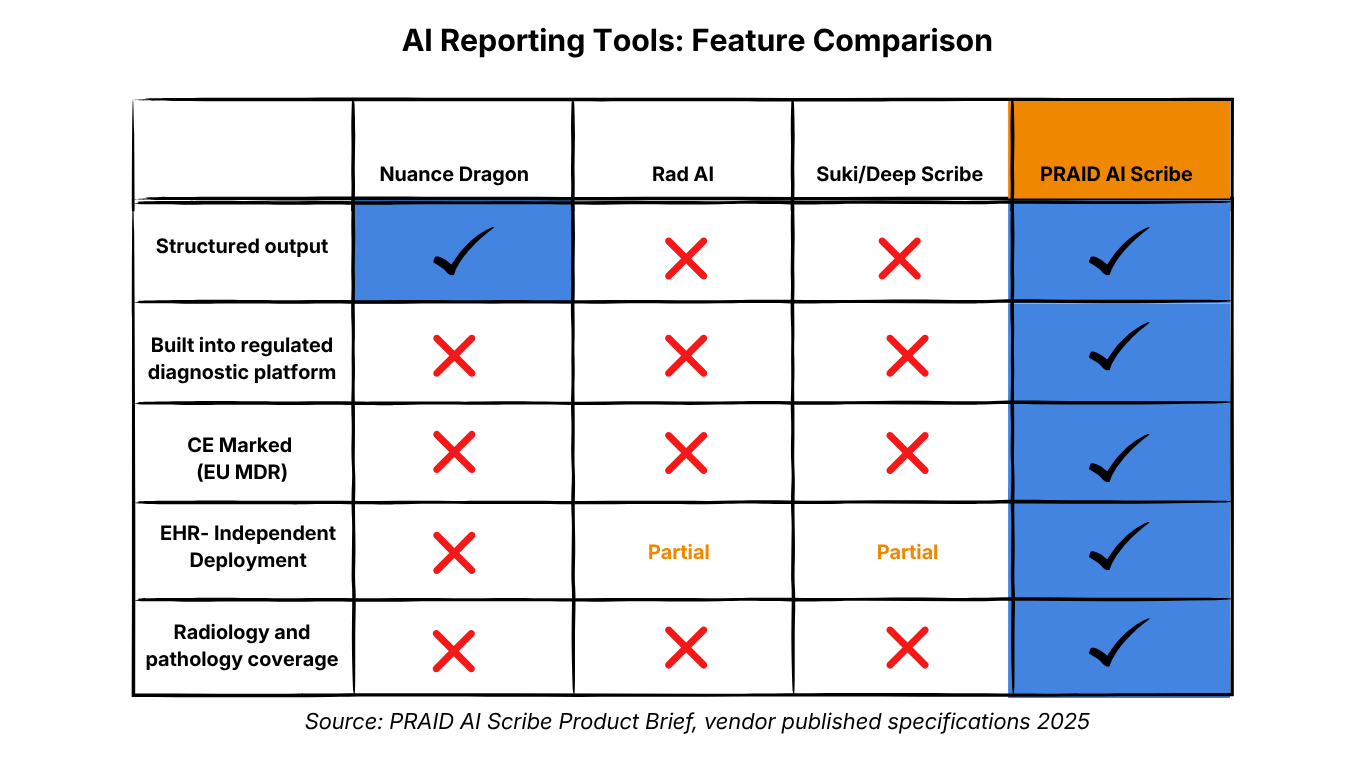
The phrase gets used a lot. But the mechanism matters, because not all AI reporting tools do the same thing — and understanding the difference is critical to buying the right solution.
A radiologist dictates. The software transcribes. The radiologist then structures the transcript — moving text into Technique, Findings, and Impression sections, formatting it to the hospital's template, correcting transcription errors, adding measurements. This saves some typing. It does not save the cognitive overhead of structuring.
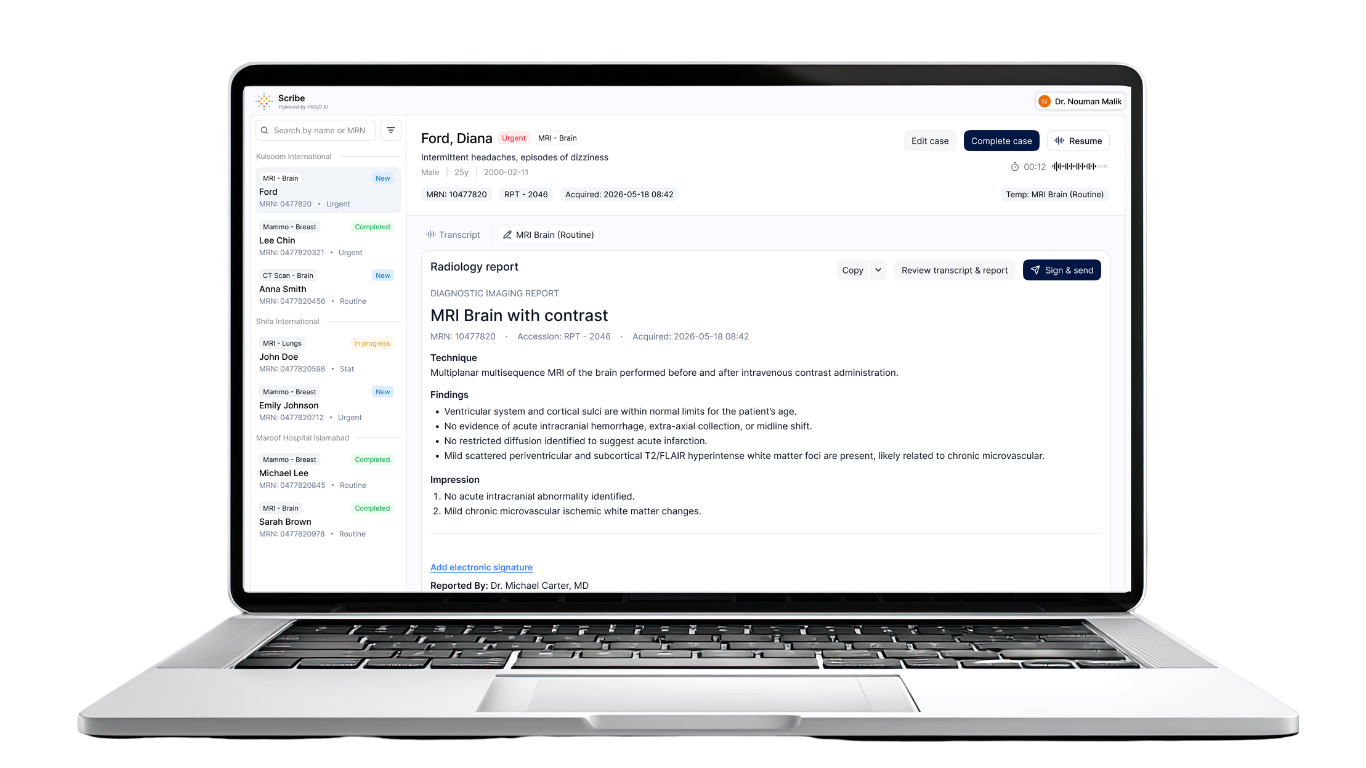
A radiologist dictates. The AI transcribes, identifies clinical terms and measurements in real time, and immediately outputs a fully structured draft — Technique populated, Findings organised, Impression drafted, aligned to the hospital's modality-specific template. The radiologist reviews, edits inline if needed, signs, and sends. End to end: under 10 seconds from end of dictation to a structured, ACR-aligned draft.
"Dragon makes the clinician type less. Scribe makes the platform think more."
This is precisely the layer PRAID AI Scribe was built to be. It is not a transcription add-on bolted onto an EHR. It is the ambient reporting layer for radiology and pathology — CE marked, ISO 13485 certified, and EUDAMED registered, with three live diagnostic models already deployed across hospitals.
The distinction is not trivial. In a department doing 200 studies per day, the difference between transcription and structured drafting compounds across every report, every shift, every radiologist. The time savings are real. But cognitive relief — not having to hold a mental template while you dictate — is arguably more valuable.
For radiologists, the burnout argument is sufficient. For CMOs and procurement leads, there is a parallel case that deserves equal weight: regulatory risk.
Many AI reporting tools currently marketed to hospitals outside the United States carry HIPAA compliance as their primary credential. HIPAA is a US data privacy standard. It is not a device safety or clinical accuracy certification. Deploying a HIPAA-scoped tool in a GCC, European, or regulated emerging-market hospital does not satisfy the procurement and liability requirements those markets actually enforce.
PRAID AI Scribe is CE Marked under EU MDR, ISO 13485:2016 certified, and EUDAMED registered.
These are device-grade certifications — the standard that procurement committees in the EU, GCC, and comparable markets require and that create a defensible compliance position in a clinical audit. The regulatory moat is not a badge. It is operational protection for the hospital.
One of the most common objections to AI adoption in clinical settings is scope: "We are not ready to replace our PACS," or "We cannot go through a full platform migration." It is a reasonable concern. Most AI radiology tools are bundled into larger platform plays that require significant infrastructure commitment.
PRAID AI Scribe is now available as a standalone application. If your department's only immediate need is faster, structured, human-reviewed reports — without touching your existing PACS, LIS, HIS, or RIS infrastructure — Scribe is the answer. It sits over the workflow you run today. No rip and replace. No retraining. No IT project.
For radiology departments that want the reporting fix now and the broader diagnostic platform later, Scribe is the entry point. The intelligence upgrades. Everything else stays exactly as it is.